Role of Endoscopic Stricturotomy in Management of Inflammatory Bowel Disease Associated Strictures

Gianna Baker, MS
Division of Gastroenterology, Hepatology and Nutrition, Allegheny Health Network
Pittsburgh, Pennsylvania, USA

Sandra El-Hachem, MD
Division of Gastroenterology, Hepatology and Nutrition, Allegheny Health Network
Pittsburgh, Pennsylvania, USA

Gursimran Singh Kochhar, MD, FACP, CNSC
Associate Chief, Division of Gastroenterology, Hepatology and Nutrition, Allegheny Health Network Medical Director, Endoscopic Innovations, Allegheny Health Network Assistant Professor of Medicine, Drexel University Pittsburgh, Pennsylvania, USA
Case: A 32-year-old Caucasian female who is nine months postpartum and breastfeeding presents to the hospital with nausea and vomiting lasting for five days. She has a history of ileocolonic Crohn’s Disease (CD) with ileocecal resection five years prior with primary ileocolonic anastomosis. On admission, her CT scan indicates an anastomotic stricture, 1 cm in length, with mild prestenotic dilation. The patient’s only current outpatient medication is adalimumab. Upon physical exam, her abdomen is slightly distended, soft, and tender with bowel sounds present. Endoscopy reveals stenosis involving the ileocolonic anastomosis (Image 1). The patient then undergoes endoscopic balloon dilation (EBD) of 15 mm. Patient was subsequently discharged. Four weeks later, she presented with similar symptoms and was admitted with partial small bowel obstruction. In this scenario, how would you proceed?
A. Send the patient to surgery
B. Repeat endoscopic balloon dilation, consider steroid injections post-dilation at the dilation site
C. Switch patient to a different biological medication from adalimumab
D. Perform an endoscopic stricturotomy
Inflammatory bowel disease (IBD) affects 0.5% of the population, translating to over one million individuals in the US with this diagnosis.1 Its compounding prevalence is expected to result in an exponential increase of diagnoses within the next few years, prompting the medical community to seek out innovative treatments to improve management strategies.1 CD can result in various complications, one of them being stricture formation. Although the exact cause of stricture formation is unknown, untreated chronic inflammation is thought to be the primary driver of the stricture formation.2 The most common location for stricture formation in CD patients is the small bowel, followed closely by the anastomoses and tends to follow the distribution of inflammation.2 Although surgical resection is the most definitive treatment, it can be associated with complications. EBD has been used for quite some time to manage the strictures and delay need for surgeries. Recently a new technique, endoscopic stricturotomy (ESt), has been developed to treat these strictures endoscopically.
In 2017, Lan and Shen first described their experience using ESt for the treatment of strictures in patients with IBD.5 ESt is an innovative procedure, one in which strictures are cut with electroincision knives in either a radial, horizontal, semi circumferential, or circumferential fashion.5,6 In this technique, if the incised edges are closed with clips, it is referred to as endoscopic stricturoplasty. If no clips are deployed, it is described as endoscopic stricturotomy.7
This procedure offers significant precision due to the endoscopist controlling the cutting length and depth of strictures. Since the inception of ESt, multiple studies regarding the technique’s efficacy and safety have been conducted (Table 1). These studies have demonstrated technical success rates as high as 92%7 and 100%.5 The risk of perforation seems to be low; however, the risk of post-procedure bleeding is high (Table 2).5,8 Although early, these results have demonstrated the efficacy of utilizing ESt over the surgical procedures or EBD in the management of strictures in a select group of patients.
When compared to other modalities of treatment ESt seems to be as effective as the existing therapeutic options. In one study, EBD and ESt were compared. A total of 185 CD patients with anastomotic strictures were included; the technical success rate was 100% for patients receiving ESt and 89.5% for patients receiving EBD (P = 0.25).8 This group also found that ESt patients experienced both a higher rate of symptomatic and endoscopic improvement than EBD patients, although this did not reach statistical significance. Additionally, only 9.5% of ESt patients were required to undergo subsequent salvage surgery compared to 33.5% of EBD patients that required salvage surgery (P = 0.03). When it came to ileo-colonic resection (ICR), ESt was found to be equally effective. In a study by Lan et al. that compares ESt and ICR in treating anastomotic strictures, it was found that ICR patients experienced significantly more postprocedural adverse events than ESt patients (31.9% vs. 10.2%, P = 0.003).9 It was also reported that patients who underwent ICR had overall higher morbidity and subsequent disease-related hospitalizations than ESt patients. Though not statistically significant, only 8.3% of ESt patients required salvage surgery, whereas 16.7% of ICR patients required secondary surgery (P = 0.54).9 In another study, post-procedural adverse events, such as perforation and infection, were significantly more frequent in patients that underwent ICR as compared to those that underwent ESt (P = 0.05).10
Recently the Global Interventional IBD Group (co-founded by Bo Shen and GS Kochhar) has proposed the consensus guidelines on the management of strictures endoscopically. The guidelines state, EBD remains the first line treatment modality for treating strictures endoscopically; the role of ESt is emerging. The guidelines prefer ESt over EBD for treatment of severe fibrotic strictures or strictures of the distal bowel due to the advantage of the endoscopist having complete control of the depth and location of the electroincision. Additionally, the group believes that this technique is preferable in the management of nonangulated, short fibrotic strictures. Though this technique is more demanding than EBD because of its required expertise and is documented to impose a higher risk of post-procedural bleeding, ESt may be more effective in reducing the need for eventual surgery. Therefore, they propose that interventional IBD training be incorporated into the curriculum of the fourth-year advanced endoscopy fellowship or fourth-year IBD fellowship to properly train the future generations of IBD interventionalists to utilize such complex endoscopic techniques accordingly.7
Here at our center for interventional IBD, we have performed 75 endoscopic stricturotomies thus far. The locations of strictures include the upper GI tract, small bowel, colon, and anal strictures. The technical success of the procedures was 98.6%, with a rate of adverse events of 9.3% (one perforation, managed conservatively, and six patients with post-procedure bleeding). We offer this procedure to our patients in a multi-disciplinary approach.
With the rising prevalence of IBD diagnoses worldwide,1 it is essential now more than ever for medical professionals of the IBD community to pioneer innovative, minimally-invasive techniques to manage strictures resulting from this disease. Although still a novel therapy, ESt remains an up-and-coming viable and effective therapeutic option for patients with strictures. As our tools improve, the technique will improve further and become an important technique for managing our patients with strictures.
Answer to the case study: D (Image 2)
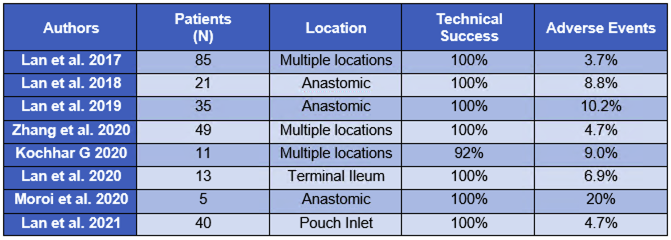
Table 1. A summary of studies on endoscopic stricturotomy in IBD.5, 6, 8, 9, 10, 11, 12, 13
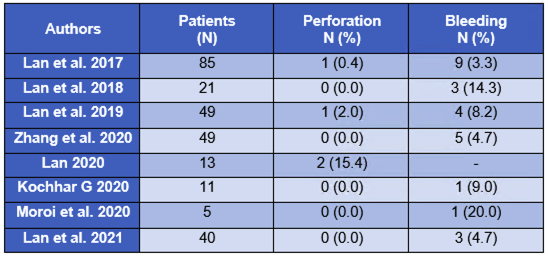
Table 2. A summary of recorded adverse events of endoscopic stricturotomy procedures.5, 6, 8, 9, 10, 11, 12, 13
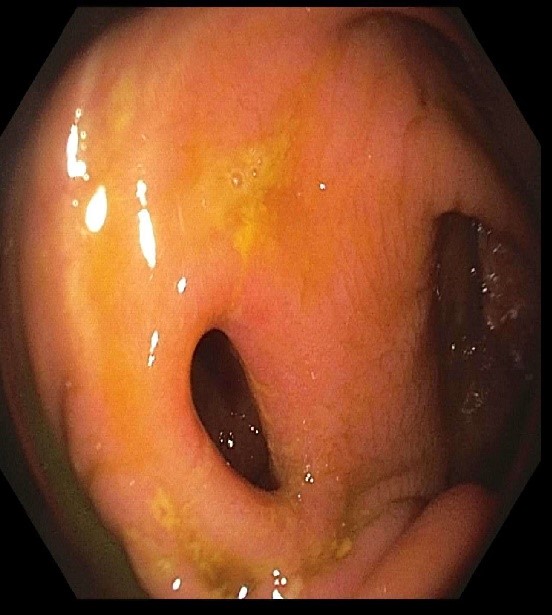
Image 1. Anastomic structure, 1 cm in length, before treatment
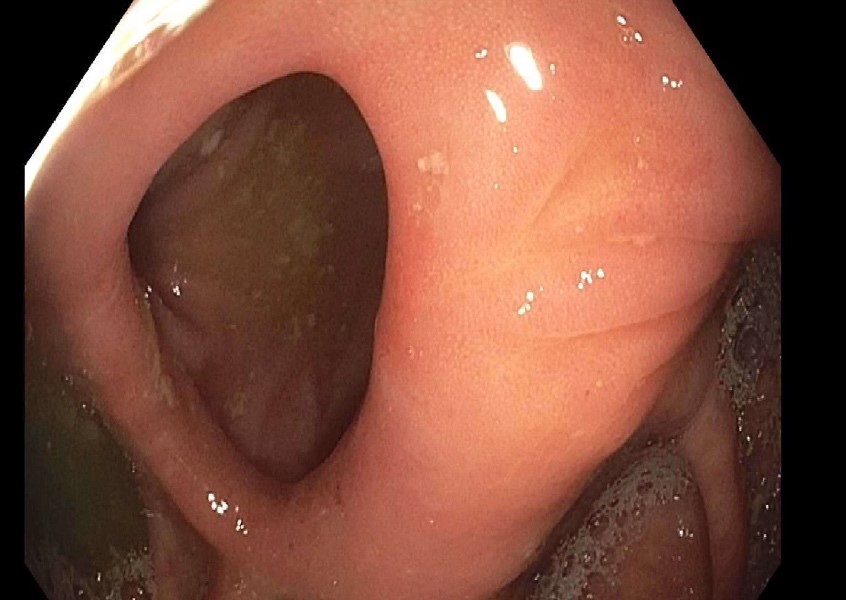
Image 2. After treating the anastomic stricture with ESt
References
1. Kaplan GG. The global burden of IBD: from 2015 to 2025. Nature Reviews Gastroenterology & Hepatology. 2015;12(12):720-727. doi:10.1038/nrgastro.2015.150
2. El Ouali S, Click B, Holubar SD, Rieder F. Natural history, diagnosis and treatment approach to fibrostenosing Crohn’s disease. United European Gastroenterology Journal. 2020;8(3):263-270. doi:10.1177/2050640620901960
3. Mohy-ud-din N, Kochhar GS. Endoscopic Stricturotomy Is an Efficacious Option for Management of Strictures in Patients With Inflammatory Bowel Disease. Crohn’s & Colitis 360. 2020;2(4). doi:10.1093/crocol/otaa069
4. Thia KT, Sandborn WJ, Harmsen WS, Zinsmeister AR, Loftus EV. Risk Factors Associated With Progression to Intestinal Complications of Crohn’s Disease in a Population-Based Cohort. Gastroenterology. 2010;139(4):1147-1155. doi:10.1053/j.gastro.2010.06.070
5. Lan N, Shen B. Endoscopic Stricturotomy with Needle Knife in the Treatment of Strictures from Inflammatory Bowel Disease. Inflammatory Bowel Diseases. 2017;23(4):502-513. doi:10.1097/MIB.0000000000001044
6. Mohy-ud-din N, Kochhar GS. Endoscopic Stricturotomy Is an Efficacious Option for Management of Strictures in Patients With Inflammatory Bowel Disease. Crohn’s & Colitis 360. 2020;2(4). doi:10.1093/crocol/otaa069
7. Shen B, Kochhar G, Navaneethan U, et al. Practical guidelines on endoscopic treatment for Crohn’s disease strictures: a consensus statement from the Global Interventional Inflammatory Bowel Disease Group. The Lancet Gastroenterology & Hepatology. 2020;5(4):393-405. doi:10.1016/S2468-1253(19)30366-8
8. Lan N, Shen B. Endoscopic Stricturotomy Versus Balloon Dilation in the Treatment of Anastomotic Strictures in Crohn’s Disease. Inflammatory Bowel Diseases. 2018;24(4):897-907. doi:10.1093/ibd/izx085
9. Lan N, Stocchi L, Delaney CP, Hull TL, Shen B. Endoscopic stricturotomy versus ileocolonic resection in the treatment of ileocolonic anastomotic strictures in Crohn’s disease. Gastrointestinal Endoscopy. 2019;90(2):259-268. doi:10.1016/j.gie.2019.01.021
10. Lan N, Hull TL, Shen B. Endoscopic stricturotomy and ileo-colonic resection in patients with primary Crohn’s disease-related distal ileum strictures. Gastroenterol Rep (Oxf). 2020;8(4):312-318. doi:10.1093/gastro/goz071
11. Moroi R, Shiga H, Kuroha M, et al. Endoscopic radial incision and cutting for Crohn’s Disease-associated intestinal stricture: a pilot study. Endosc Int Open. 2020;8(1):E81-E86. doi:10.1055/a-1027-6921
12. Lan N, Wu J-J, Wu X-R, L T, Hull, Shen B. Endoscopic treatment of pouch inlet and afferent limb strictures: stricturotomy vs. balloon dilation. Surgical Endoscopy. 2021;35(4):1722-1733. doi:10.1007/s00464-020-07562-z
13. Zhang L-J, Lan N, Wu X-R, Shen B. Endoscopic stricturotomy in the treatment of anastomotic strictures in inflammatory bowel disease (IBD) and non-IBD patients. Gastroenterology Report. 2020;8(2):143-150. doi:10.1093/gastro/goz051